Case Reports
August 19, 2014 1 Comment
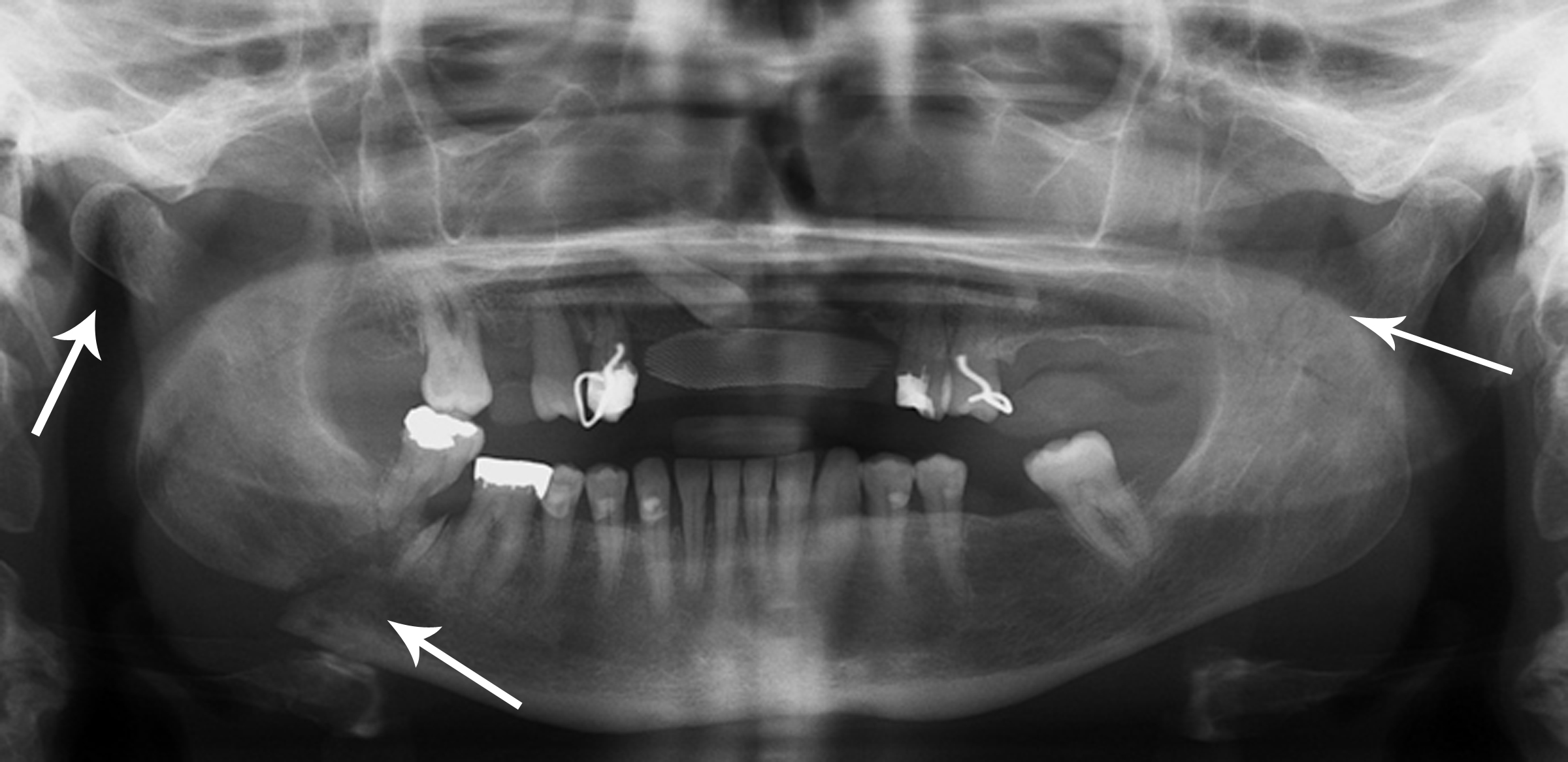
Multiple Mandibular Fractures
I am writing a chapter on facial trauma in sports and am learning quite a lot as I go.
For many of you, I am preaching to the choir when I write that teaching is one of the best ways to learn.
My charge in this chapter is to cover many aspects of maxillofacial trauma, including entities I may have dealt with infrequently, or have referred promptly and never directly handled myself (maxillofacial trauma not infrequently requires surgical intervention). That’s where the teaching–or writing in this case–as learning comes in.
I have seen my fair share of facial trauma during sideline coverage of sports. Aside from simple contusions, I would estimate that the most common entity I have to deal with is facial lacerations, followed by nasal fractures and epistaxis. But I have never conservatively managed an athlete with a frontal bone fracture.
One of the offerings in the journal that is relevant to this subject is our ‘Case Reports’ section. I think the Original Research our journal offers is our strongest suit, but the published case reports cover such a wide variety of subjects, I find that I can learn a great deal from them. This is most especially true if an author is reporting on a truly novel case or treatment. I specifically leaned heavily on a specific case report in the writing of my chapter: “Conservative Treatment in an Isolated Anterior Wall Frontal Bone Fracture in an Elite Soccer Player,” by C Eirale, R Lockhart, and C Hakim, in the 2010 CJSM.
I am citing this journal article in the writing of the chapter, as I found it to be full of useful information. Frontal bone/sinus fractures can result in serious morbidity (ranging from chronic sinus dysfunction to meningitis); surgery is often indicated. In this particular case, the authors and treating physicians felt they could treat conservatively, given that:
“(1) no posterior wall fracture on the imaging; (2) absence of cerebrospinal fluid (CSF) rhinorrhea; (3) integrity and patency of nasofrontal duct (no fracture on imaging and no signs of mucus or blood retention in the sinus); and (4) absence of laceration over the fracture (allowing a direct access for reduction and osteosynthesis).”
Rod of Asclepius
The soccer player made a remarkably quick recovery, playing a match (with facial protection) only three weeks after this serious injury. How’s that for mending the wound! Those sports clinicians would make Asclepius proud!
The journal’s Case Reports editor looks for discussions of novel pathologies or treatments. Most of our submissions are solid but must be turned away because they do not follow our strict criteria for consideration of publication for these type of reports. Our Case Report for the most recent, July 2014 CJSM is a good example of what we look for when deciding to publish. The case deals with the use of pulsed ultrasound (LIPUS) in the successful treatment of a delayed union of a hook of the hamate fracture. We thought this was an uncommon enough pathology, with a novel treatment approach, to be considered worthy of publication.
And now, I head back to writing the chapter. A September 1 deadline is looming. With football season nigh (first game is Friday evening August 29), soon enough I won’t be writing (or reading) about such injuries……I’ll be too busy handling them on the sideline!
There’s a lot coming up both in the world of sports (US Open tennis, the first kickoff of the American football season….) and the world of sports medicine (our 5th edition of CJSM for the year is about to publish). I have some great guests lined up for some upcoming podcasts. It will be a great fall. See you again soon on-line!

Pingback: The September CJSM | Clinical Journal of Sport Medicine Blog