Gender Issues in Sport: the case of Dutee Chand
October 10, 2014

Berlin Olympia Stadium: site of the 12th IAAF Athletics Championship
It’s time for a poll.
Issues of gender in sport are a regular feature in the pages of the CJSM journal and this blog.
I wanted to share with you, again, a poll that got a lot of traffic earlier this year when I wrote about the IAAF policy on gender testing in sport. The issue continues to be relevant: just this week, the New York Times published an excellent article on the subject of the Indian sprinter Dutee Chand. She is the Indian 100m women’s U18 champion, and she cannot currently compete for her country because of her naturally high testosterone levels. She faces the decision, as several female athletes have before her, of whether to retire or compete…..but the latter option is contingent on medical interventions aimed at lowering her testosterone.
The issue is highly charged, and I think both the pro and the con side of such testing and intervention make some sense in the field of competitive athletics. At the end of the day, however, I find the IAAF policy to be highly flawed. I think it is largely discriminatory, sexist, and reductionist: too high of testosterone = you cannot compete as a woman.
Read the rest of this post and take the poll. At CJSM, we’re interested to know what you think!

Clinical Journal of Sport Medicine Blog
I was taken by an editorial that I read in the New York Times this weekend: The Trouble With Too Much T. If you didn’t have the chance to see it yourself already, by all means click on the link and read this piece.
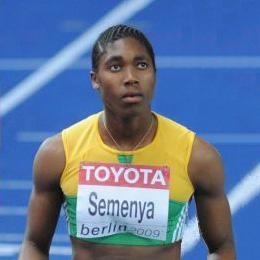 Caster Semanya, South African Olympian
Caster Semanya, South African Olympian
The authors, Katrina Karkazis and Rebecca Jordan-Young, give a broad overview of how current sports governing bodies determine if an athlete is ‘really’ female. Of note, Karkazis and Jordan-Young are also the principal authors of The American Journal of Bioethics critique of the current gender-testing policies of the IOC, IAAF and other governing bodies.
They lead with the well-known story of Caster Semanya, the South African woman who, in 2009, was barred from international competition and was compelled to undergo testing after the Berlin World Championships (she has subsequently been reinstated, and in the 2012 London Olympics was…
View original post 602 more words

