The little differences — sports medicine training in the UK
October 15, 2017

Dawn Thompson, our Junior Assoc Editor from BASEM, on a UK NICU floor!!!
Our Junior Associate editor from the British Association for Sport and Exercise Medicine (BASEM)— Dawn Thompson–joins us today with her newest contribution to the CJSM blog. As many of our regular readers know, Dr. Thompson is a sport and exercise medicine (SEM) trainee in the UK and has contributed frequently to these blog pages.
Her blog post today takes up the subject of how different SEM training can be in different sites around the world. In the USA, where I practice, one gets their primary training in a specialty such as family medicine, emergency medicine, internal medicine, pediatrics, or physical medicine & rehabilitation; only then does one pursue one to two years of further specialty training in sports medicine. New Zealand and Australia follow a very different path, as explained by the Australasian College of Sport and Exercise Physicians (ACSEP) in their website.
The UK does it their own way, and Dr. Thompson (DT) is here to tell us what that is like as she spends time on the ‘sidelines’ of the…..neonatal intensive care unit!???
_______________________________________________
DT: It’s been a busy year and a while since my last post. Once again it’s a crazy time of the morning (4am) and I’m in the midst of an unusually quiet 12.5 hour shift on the neonatal intensive care unit wondering how exactly this is going to make me a better sports physician! I’m not sure I have found the answer to that one yet but it has inspired me to think about the current state of SEM training.
Over the last 10-20 years sports and exercise medicine as its own specialty around the world has come on leaps and bounds. The UK Faculty for Sports and Exercise Medicine (FSEM) was set up in 2005 and is the governing body for SEM overseeing the training curriculum in the UK. The system in the UK is quite different to many other parts of Europe and the pathway seems to vary greatly between country and even between different states. For example, in Germany there is no dedicated training programme. Here, SEM trainees must fully qualify in a different specialty such as orthopaedics and then undertake a set number of hours of training in a sports club or SEM centre. In other countries there is no designated training pathway or what does exist lacks structure.
The UK Faculty of Sports and Exercise Medicine is currently working on developing an international base syllabus for countries which lack a SEM specialist training programme – a programme known as the Delphi programme. Information on this programme was presented at the BASEM conference in Bath, England this month and if it succeeds we can hope that in the future more and more countries will be able to develop their own training structure.
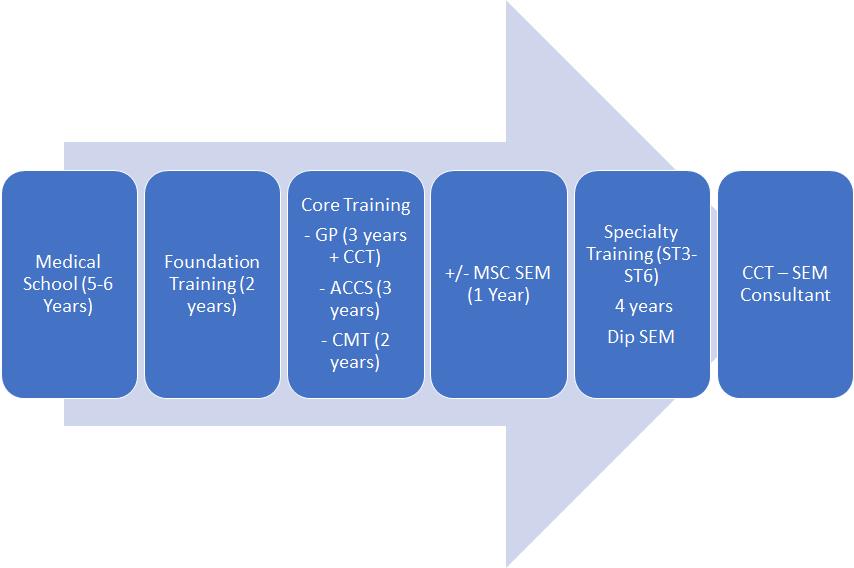
SEM Training Flow Chart
So what is the state of play in the UK and how will looking after teeny-tiny babies in the middle of the night help me get there?! Well, after much deliberation over which career path is for me, I am currently in the middle of training for a role in general practice – one of the preferred routes into Sports and Exercise Medicine in the UK. For juniors wanting to pursue this career path, the FSEM recommends entry into specialty training via one of 3 routes – General Practice, Acute Care Common Stem or Core Medical Training. At the end of this period of core training candidates can then apply for specialty training in SEM. Training posts last 4 years covering a range of specialties related to Sports and Exercise medicine including rheumatology, A+E, GP, rehab medicine, public health, general medicine and MSK medicine. At the end of the 4-year period, trainees who have passed the FSEM diploma examinations (DipSEM) consisting of 2 written papers and a 12 station OSCE will be awarded their completion of training and consultant status allowing them to become a fellow of the FSEM (see flow chart).

Dr. Thompson — life outside the NICU
The specialty training posts are highly competitive and most trainees carry out a SEM masters prior to applying in-order to increase their chance of successfully gaining a training number. In the UK there are a wide range of MSCs to choose from with classroom or home study and full or part time options. Many also include clinical attachments giving hands on experience and research projects that can lead to publications/presentations. Details on some of these courses can be found here and here.
There is much debate over the best route into specialty training and in reality it is probably down to personal preference. I chose the GP pathway as for me it is also important to be able to deal with the routine general health queries athletes may have in addition to sports specific problems. Particularly when travelling with a team, the medic will be responsible for all the health needs of the athlete and coaching team including coughs/colds and upset stomachs! Not only this but being one to always hedge my bets, training as a GP means that at the end of 3 years I will be a fully qualified GP. At least if one of those elusive registrar training posts doesn’t come my way, I will still have my completion of training in general practice and can chose to practice with a special interest in musculoskeletal medicine!
It all seems a long way off and who knows if the pathway will change before I get there. For now though its neonates for me and another baby calling – I’ll try to be in touch sooner next time!
