Computerized Neurocognitive Testing in the Management of Concussions, Part 2
August 25, 2013

Concussion management for football,
c. 1930
I woke up this morning to my usual Sunday routine: the New York Times Sports page and coffee.
Today’s sports section–and I don’t think the Times is alone in this regard–is devoted to the subject of the forthcoming American college football season. The first games of the season will take place this Thursday, August 29. As the Times puts it, “The nation’s annual rite of mayhem and pageantry known as the college football season begins this week…..”
When I’m not doing work with the Clinical Journal of Sports Medicine, I’m taking care of youth, high school and college athletes; for my colleagues and me, the football season has already begun, with the various teams we cover already having had weeks of steady, increasingly intense practices and scrimmages. And we’re seeing the injury results of the sport, including an increase in volume of concussions.
I’ve mentioned this in my blog posts for this month, where the theme has been ‘concussions.’ Last week I wrote about the special set of CJSM concussion research articles we have made freely available for a limited time. At the beginning of the month, I authored a post on the subject of computerized neurocognitive testing (e.g. ANAM4, CNS-Vital Signs, AxonSports, ImPACT, etc.) and their use in managing concussions. I want to return to that subject in today’s post.
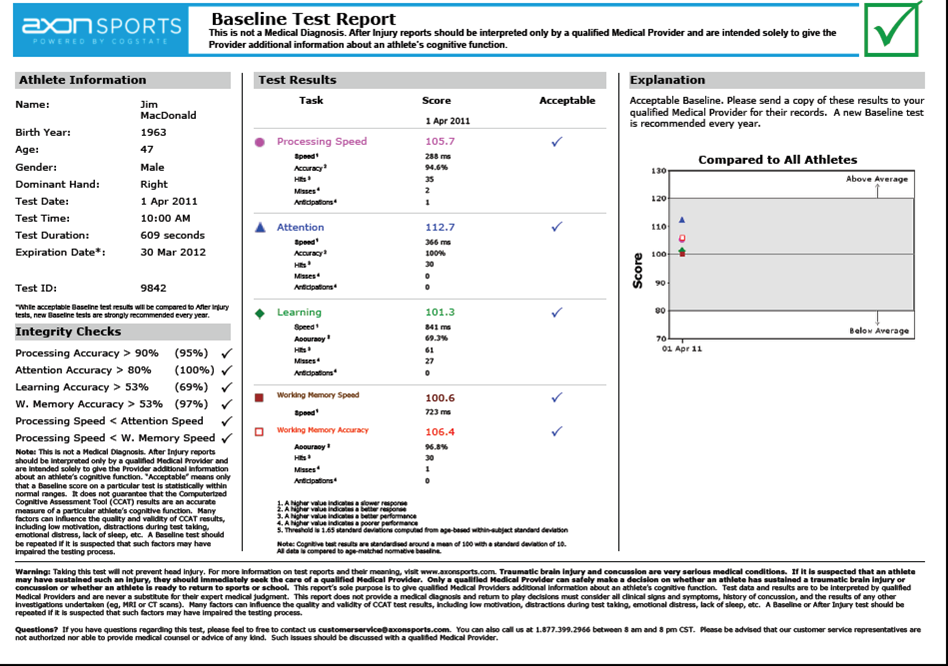
The author’s baseline AxonSport report
A recent article from the Archives of Clinical Neuropscyhology was especially interesting, I thought. The authors looked at a military population while evaluating the test-retest reliability of four computerized neurocognitive assessment tools (NCATs): Automated Neuropsychological Assessment Metrics 4 (ANAM4), CNS-Vital Signs, CogState (available now in the U.S. as ‘Axon Sports’), and ImPACT). I’m familiar with these products, but most especially ‘know’ CogState, as this is the NCAT we use in our clinic.
The authors correctly assert that test-retest reliability is one of the “…fundamental psychometric characteristics that should be established in each NCAT,” and that “….reliability should be established before making conclusions about a test’s validity,” which is the psychometric construct that can indicate whether a test measures what one is truly trying to measure (for instance, ‘reaction time,’ or ‘memory’). Reliability, is the “…extent to which the test produces consistent results across multiple administrations to the same individual.”
In this study of 215 individuals (mean age 34, range 19 to 59), Read more of this post






